PRF vs PRP. Which one is better?
One of the most common question when it comes to accelerated soft and hard tissue healing boosters.
The short answer is PRF. If you would like to find out why, keep reading this article.
Advantages that shows to PRF compared to PRP and PRGF:
- greater simplicity of production
- absence of blood manipulation
- no additives
- PRF produces a larger share of blood product over the share of blood taken
- contains more healing factors
- more stem cells, less trauma
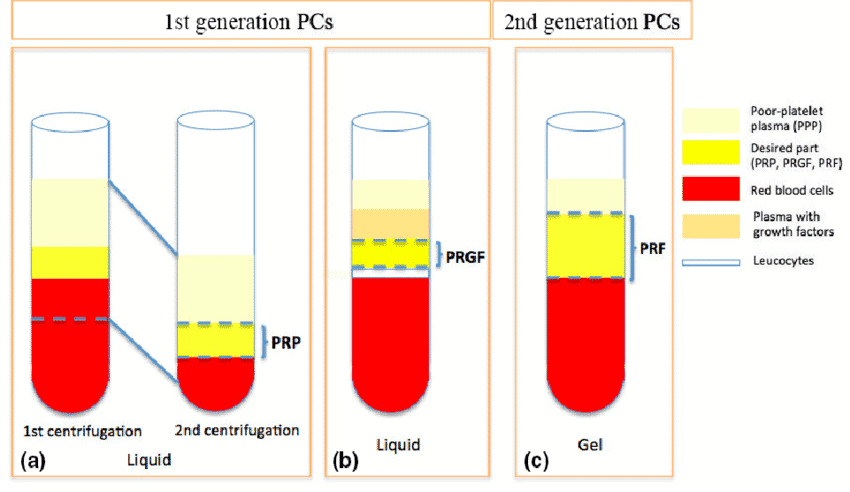
Generation of platelet concentrates: PRF vs PRP vs PRGF
Many efforts have been made to find new and specific “bioactive” additives that promote and accelerate wound healing, regulate inflammation, and improve soft and hard tissue regeneration. The most common are PRP, PRGF and PRF techniques.
Platelet-Rich Fibrin – PRF- is a second generation platelet concentrate. PRF was subsequently introduced by Dr. Joseph Choukroun inventor of PRF and his co-workers in 2001.
PRF is a 100% autologous biomaterial, it accelerates wound healing and tissue regeneration, increases stimulation of osteogenesis and new blood vessel formation. PRF contains approximately 10 times more platelet concentration than normal blood, therefore having great healing and regenerative properties.

PRP
Platelet-rich plasma (PRP) is a first generation platelet concentrate aimed to improve tissue repair. It is a gel at high concentration of autologous platelets suspended in a small amount of plasma after centrifugation of the blood of the patient. PRP has some significant disadvantages: the preparation protocol is expensive, complicated, and very operator-dependent, and the need for animal thrombin as a coagulant raises legal issues in some countries.The short duration of cytokine release and its poor mechanical properties have resulted in search of new material.
PRGF
Plasma Rich in Growth Factor (or PRGF) is a type of plasma enriched of proteins and circulating growth factors able to aid the bone and soft tissue regeneration. PRGF contains many different cells and cell-types highly concentrated in a gelatinous form which can be placed into the site of the injury: these cells stimulate and accelerate the healing process by forming blood clots and releasing growth factors into the wound. PRGF does not need bovine or human thrombin for coagulation, however it necessitates Calcium Chloride to be added to PRGF. PRGF includes plasma proteins and coagulative factors and is then more advantageous compared to PRP.
PRF
Platelet Rich Fibrin (PRF) is a modern, natural platelet concentrate, it is achieved with a simplified preparation, with no biochemical manipulation of blood. This technique does not require anticoagulants or bovine thrombin (or any other gelling agent). This feature makes this product easily usable, with a low rate of mistakes during the preparation stage. The blood taken, approximately 10 ml in tubes without anticoagulant, is immediately centrifuged. The fibrinogen is initially concentrated in the upper part of the tube but, upon the contact with thrombin normally present in the blood, it is converted into fibrin. The platelets are retained into the meshes of fibrin.
PRF course with the inventor Dr. Joseph Choukroun
25-26th March, 2022 London
- Dr. Choukroun’s upcoming Platelet Rich Fibrin -PRF- course is an enlightenment on the biological and mechanical conditions for long term stability and success of bony and soft tissue management.
- Learn about PRF use in dental implantology, oral surgery, bone graft. Prepare PRF products on the hands-on session, practice phlebotomy and start utilising PRF from the next day in your dental practice.

Difference between PRF vs PRP
PRF stands out as a superior treatment option.
Both products require blood to be taken from the patient. PRP requires more blood to be taken than PRF. Both of the products require the whole blood sample to be placed into a centrifuge, where the blood is then processed to help separate the blood into distinct layers. PRP is spun at a higher speed, which effectively causes all of the heavier cells in the blood, such as white blood cells and stem cells, to collect in the bottom part of the test tube and allows the lighter platelets and plasma to collect in the top part of the test tube. The platelets and plasma are then collected from the upper part of the test tube and injected into the region with tissue damage.
The PRF product is spun at a lower speed so that the layers of the blood do not separate out as distinctly. This allows some of the white blood cells and stem cells to remain within the platelet layer that is collected for treatment. Thus, there are more healing factors within PRF than is typically seen in PRP. In addition, the lower spin speed causes less trauma to the individual cells of the blood, allowing more stem cells to remain in the final PRF product.
With PRF, no anticoagulant is used during the processing of the blood. With PRP, the blood that is collected is placed in test tubes that have an anticoagulant called acid citrate dextrose (ACD), which keeps the blood product from clotting too quickly. In an effort to keep the platelet product as natural as possible, the PRF tubes do not have any anticoagulant within them.
PRF is able to stimulate osteogenesis in bone environment, in addition to angiogenesis.

The benefit of using the first generation of platelet concentrates was very much debatable and the subject of controversy, but the second generation – PRF – produces more consistent and predictable results. The advantages of using PRF vs PRP are its autologous nature, simple collection, ease of chair-side preparation, and simple clinical application without the risks associated with allogeneic or animal derived products. The biological properties of PRF clearly show an interesting surgical versatility and all the characteristics that can support faster tissue regeneration and high-quality clinical outcomes.
All these features support the conclusion that the PRF is the best blood productable to better enhance the healing of soft and hard tissue, comparing to other similar blood product.
If you liked this article check out our social media pages for more content.
References:
S. GIANNINI A. CIELO, L. BONANOME, C. RASTELLI, C. DERLA, F. CORPACI, G. FALISIComparison between PRP, PRGF and PRF: lights and shadows in three similar but different protocols
Ana Castro, Nastaran Meschi, Andy Temmerman, Nelson R. Pinto: Regenerative potential of Leucocyte- and Platelet Rich Fibrin (L-PRF). Part A: intrabony defects, furcation defects, and periodontal plastic surgery. A systematic review and meta-analysis
